ESG represents a safe, minimally invasive and versatile intervention for obesity
- owenhaskins
- Feb 24
- 5 min read
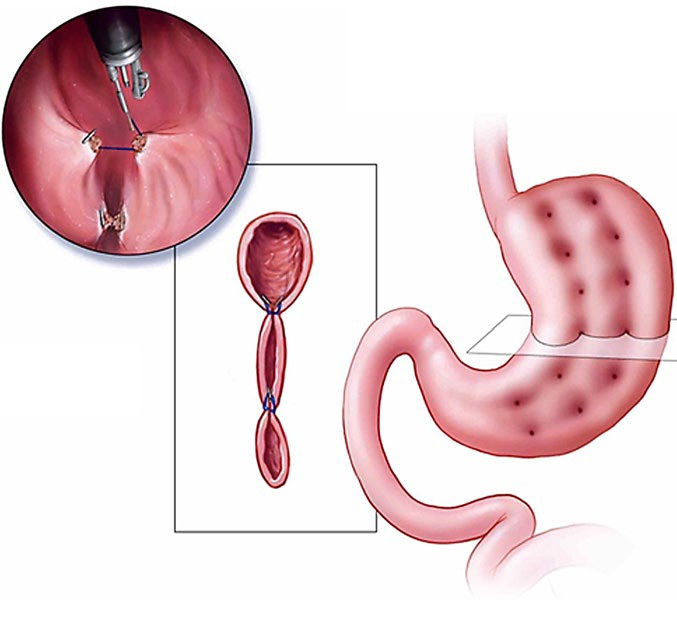
A qualitative narrative review by researchers at St George’s University, St George’s, Grenada, has reported that endoscopic sleeve gastroplasty (ESG) represents a safe, minimally invasive and versatile intervention for obesity, occupying a unique position between conservative medical therapy and surgical bariatric procedures.
According to the researchers, their review highlights ESG’s ability to produce meaningful weight loss and metabolic improvements while minimising procedural risk, preserving gastric anatomy and enabling faster recovery. Comparative analyses suggest that while surgical approaches, such as laparoscopic and open sleeve gastrectomy, achieve greater absolute weight loss, ESG offers a favourable balance of efficacy, safety, and procedural flexibility, making it particularly suitable for patients with moderate obesity, a higher surgical risk, or a preference for non-permanent interventions.
Despite growing ESG utilisation, heterogeneity persists in reported outcomes, technical approaches and patient selection criteria across studies, and direct comparisons between ESG and established surgical bariatric procedures, particularly laparoscopic sleeve gastrectomy (LSG), continue to evolve as longer-term and real-world data emerge. Therefore, the researchers sought to clarify the role of ESG within modern obesity treatment algorithms and to delineate its strengths, limitations and areas requiring further investigation.
Patient selection
The authors stated that candidate selection should incorporate comorbidity assessment, including type 2 diabetes, hypertension, dyslipidaemia, and non-alcoholic fatty liver disease. ESG has been shown to improve metabolic parameters, including reductions in glycated haemoglobin (HbA1c) and blood pressure, which supports its use in patients seeking both weight reduction and comorbidity management. Ideal candidates are motivated, able to adhere to post-procedural lifestyle changes, and free of contraindications to endoscopy or general anaesthesia.
Contraindications include severe gastroesophageal reflux disease, large hiatal hernia, prior gastric surgery altering anatomy, coagulopathy, or active peptic ulcer disease. Psychiatric assessment may also be considered to ensure realistic expectations.
Indications
Emerging indications for ESG include bridge therapy for high-risk surgical candidates, revisional therapy for post-bariatric weight regain, and combination with pharmacologic therapies, such as glucagon-like peptide-1 (GLP-1) receptor agonists, to optimise weight loss and metabolic outcomes. The consideration of gastric anatomy, prior surgical history and behavioural readiness is essential in tailoring patient selection. Shared decision-making remains critical, balancing procedural efficacy, safety and patient preferences to maximise both short- and long-term outcomes.
Safety profile
Endoscopic sleeve gastroplasty (ESG) is generally well-tolerated, with a favourable safety profile compared to surgical bariatric procedures. Across multiple prospective and multi-centre studies, serious adverse events are reported in approximately 1%-2% of cases, while minor adverse events such as transient pain, nausea or vomiting occur in 15%-20% of patients. Most minor complications are self-limited and resolve within a few days with conservative management.
The most common serious complications include gastrointestinal bleeding, perigastric fluid collections, and, rarely, gastric perforation. Pulmonary complications are uncommon but can occur, primarily related to anaesthesia in high-risk patients.
Compared to LSG, ESG avoids stapling, gastric resection and permanent anatomical alteration, contributing to lower rates of severe complications, shorter procedural times and faster recovery. Additionally, ESG does not appear to increase the risk of nutritional deficiencies commonly associated with malabsorptive bariatric procedures, although adherence to post-procedural dietary guidance remains critical.
Operator experience and procedural volume are important determinants of safety. Centers with established ESG programmes report reduced complication rates and improved technical efficiency, highlighting the role of standardised training and experience in minimising adverse events. Careful patient selection, including the evaluation of comorbidities, prior abdominal surgery, and gastric anatomy, further reduces procedural risk.
Clinical outcomes
According to the authors, ESG has consistently demonstrated clinically meaningful and durable outcomes across short-, medium-, and long-term follow-up, establishing it as a central tool in contemporary obesity management. In the short term (6-12 months), ESG achieves total body weight loss (TBWL) of 15%-20% and excess weight loss (EWL) of 50%-60%, with reductions in BMI averaging 5-7 kg/m². Patients also experience significant metabolic improvements, including reductions in HbA1c (0.8%-1.2%), fasting glucose, triglycerides, low-density lipoprotein cholesterol, systolic blood pressure, and inflammatory markers such as C-reactive protein, reflecting the procedure’s impact on both weight and cardiometabolic risk. Procedural success rates are high (>95%), and the incidence of serious adverse events is low, supporting ESG as a safe and effective intervention in the early post-procedural period.
Medium-term outcomes (12-24 months) demonstrate the maintenance of 13%-18% TBWL and sustained metabolic benefits. Longitudinal studies report that 80%-85% of patients retain ≥10% TBWL at 24 months, with most comorbidities, including type 2 diabetes and hypertension, remaining improved. Patient-reported outcomes also indicate increased satiety, improved mobility, and enhanced quality of life, highlighting ESG’s broader functional and psychosocial impact. A modest weight regain may occur in a subset of patients, underscoring the importance of adhering to structured dietary, behavioural and follow-up programmes.
Long-term outcomes, extending up to five years in emerging data, suggest durable weight reduction in 50%-60% of patients, with continued improvement in metabolic markers and low rates of revisional intervention. Weight regain, when present, is generally modest and may be mitigated through adjunct pharmacologic therapy, such as GLP-1 receptor agonists, or repeat endoscopic plication. Predictors of long-term success include a lower baseline BMI, greater adherence to lifestyle modifications, an optimal suture pattern and number, an early response to ESG, and the combination with pharmacotherapy.
When compared to intensive lifestyle modification or pharmacologic therapy alone, ESG consistently achieves superior weight loss and metabolic improvement. Relative to LSG, ESG produces slightly lower absolute weight loss but offers advantages including a minimally invasive approach, the preservation of gastric anatomy, lower complication rates, shorter recovery times, and the potential for reversibility. Collectively, these data (as depicted in Table 2) establish ESG as a practical, durable, and versatile intervention, providing meaningful clinical, metabolic, and quality-of-life benefits across short-, medium-, and long-term horizons.
Another key advantage of ESG is its reversibility and procedural flexibility. Gastric anatomy is preserved, allowing for repeat endoscopic plication in cases of weight regain and combination with adjunct pharmacologic therapy (e.g., GLP-1 receptor agonists). Surgical sleeves are permanent, and revisions require higher technical complexity with increased risk. ESG can also serve as a bridge to surgery for high-risk patients, enabling preoperative weight loss to reduce operative risk.
“Integrating ESG into healthcare systems and cost-effectiveness analyses is a crucial priority. Understanding how ESG fits within multidisciplinary obesity management, including its impact on recovery, procedural risk, and combination with pharmacologic therapy, will inform clinical decision-making and facilitate broader adoption. Emerging applications, including combination with pharmacologic therapies, use as a bridge to surgery, and revisional strategies for post-surgical weight regain, underscore ESG’s expanding clinical relevance,” the authors concluded. “Future research, focusing on procedural refinement, long-term outcomes, optimised patient selection, and integration into multidisciplinary care pathways, will further define its role in contemporary obesity management.”
The findings were featured in the paper, ‘Endoscopic Sleeve Gastroplasty: A Qualitative Narrative Review of Outcomes, Safety, and Clinical Applications’, published in Cureus. To access this paper, please click here



Comments