POWER: The next chapter of obesity care
- owenhaskins
- Jul 5
- 3 min read
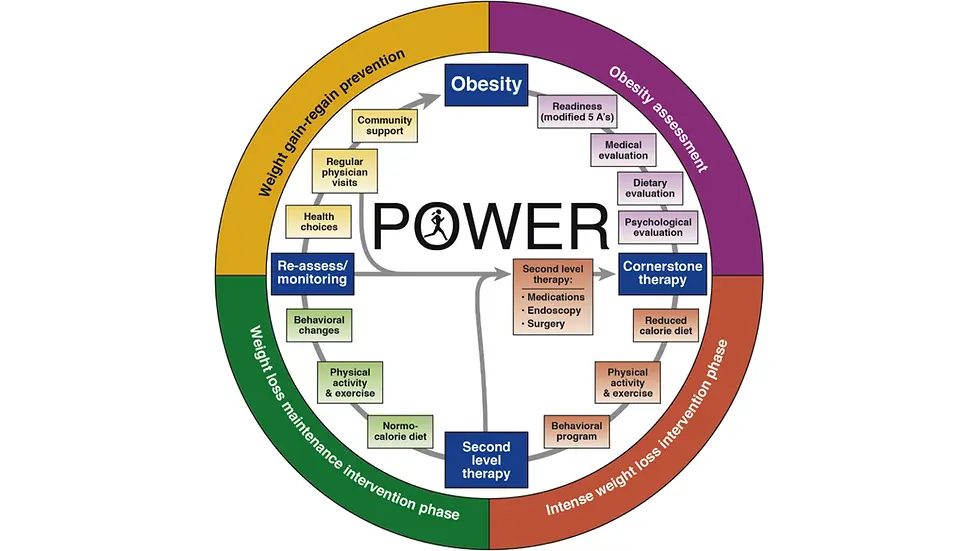
The rapid rise of GLP-1 medications such as semaglutide and tirzepatide has transformed obesity treatment. Still, experts say medications alone are not enough to address one of the US’ most pressing chronic diseases. A commentary published in Gastroenterology, "Revisiting POWER in the GLP-1 Age," updates the landmark POWER (Practice Guide on Obesity and Weight Management, Education, and Resources) framework first published in 2017.
The paper reflects major advances in obesity care, including the emergence of highly effective anti-obesity medications, new evidence supporting endoscopic bariatric and metabolic therapies, expanded indications for bariatric surgery, and advances in precision medicine.
Key takeaways:
GLP-1 receptor agonists have fundamentally changed the treatment landscape for obesity.
The commentary incorporates the emerging concept of clinical obesity, which recognizes obesity as a chronic, systemic disease and highlights the limitations of relying on body mass index alone to assess health risks.
Obesity care is increasingly moving toward a multidisciplinary model that combines medications, endoscopic therapies and surgery.
New evidence supports endoscopic sleeve gastroplasty and other endoscopic bariatric and metabolic therapies as effective treatment options.
Advances in genetics and precision medicine may help physicians better match patients with obesity treatments that are most likely to be effective.
Combining GLP-1 medications with endoscopic or surgical interventions may produce greater and more durable weight loss than either approach alone.
The paper emphasises the important role gastroenterologists and hepatologists play in obesity management. These specialists routinely care for patients with obesity-related conditions such as metabolic dysfunction-associated steatotic liver disease (MASLD), gastroesophageal reflux disease (GERD), gallbladder disease, and gastrointestinal complications associated with obesity.
Bariatric surgery
The paper states that bariatric surgery remains the most safe, effective, and enduring treatment for patients with obesity and significant weight-related comorbidities. Long-term data have demonstrated the success of MBS in terms of both durable excess weight loss and improvement in weight-related medical diseases. In addition, perioperative and long-term safety evaluations have demonstrated low rates of minor and major complications, as well as decreased mortality, cost, and failure to rescue postsurgical complications, when MBS is performed by experienced surgeons in a comprehensive bariatric treatment center, particularly those accredited through the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program.
Long-term studies assessing the weight loss outcomes of bariatric surgery have demonstrated improvement in all-cause survival compared with cohorts with severe obesity and weight-related disease that did not undergo surgical intervention. A meta-analysis of more than 174,000 patients calculated a 6.6 million increase in potential life-years for every 1% increase in MBS use. Another systematic review and meta-analysis of 12 survival studies reported an overall 5-year median reduction in mortality of 38% for patients who underwent MBS vs those who did not.
In their jointly issued 2022 guidelines, the American Society for Metabolic and Bariatric Surgery and International Federation for the Surgery and Other Therapies for Obesity recommended MBS for individuals with BMI > 35 kg/m2, regardless of the presence, absence, or severity of comorbidities, and in patients with type 2 diabetes with BMIs of 30–34.9 kg/m2; MBS should also be considered in individuals with BMIs of 30–34.9 kg/m2.5 Overall, perioperative mortality for bariatric surgery is 0.1%, which is lower than for hernia repair and cholecystectomy. Patients undergoing MBS should undergo nutritional status assessment prior to surgery, as many patients have preoperative nutritional deficiencies.
The three most performed primary MBS operations in the US are laparoscopic sleeve gastrectomy, Roux-en-Y gastric bypass, and duodenal switch. The laparoscopic sleeve results in 25%–30% TBWL with concomitant improvement of weight-related comorbid conditions. Roux-en-Y gastric bypass results in 30%–35% TBWL with overall reductions in comorbidities. The duodenal switch results in excellent weight loss (TBWL 40%) but places the patient at risk for nutritional deficits, including protein and fat-soluble vitamins D, E, A, and K deficiencies.
The paper also states that combining GLP-1s with ESG or other endobariatric and surgical interventions yields superior outcomes to monotherapies, with better long-term outcomes. Such a multidisciplinary stepped-care approach takes into account the chronic nature of obesity and reinforces the principles of the original POWER model.
The paper strongly recommended that gastroenterologists and hepatologists embrace the management of obesity: “Gastroenterologists’ and hepatologists’ position at the front line of the obesity epidemic allows them to combine endoscopic procedures with novel medications to treat obesity and related GI diseases. The prospect of novel and, it is hoped, reimbursable procedures points to a bright future for obesity management, one in which practitioners can take advantage of a continuously growing medicinal toolbox and an exciting path toward precision obesity care. Therefore, POWER 2.0 is a live document with state-of-the-art information to adopt obesity care in your practice.”
The white paper, ‘Revisiting POWER in the GLP-1 Age’, was published in Gastroenterology. To access the paper, please click here



Comments