
Extended pouch RYGB results in better weight loss outcomes standard RYGB
- owenhaskins
- Feb 16
- 4 min read
Extended pouch gastric bypass (EP-RYGB) results in slightly better weight loss outcomes and similar health-related quality of life (HRQoL) compared to standard Roux-en-Y gastric bypass (S-RYGB) five to nine years postoperatively, according to researchers from the Netherlands.
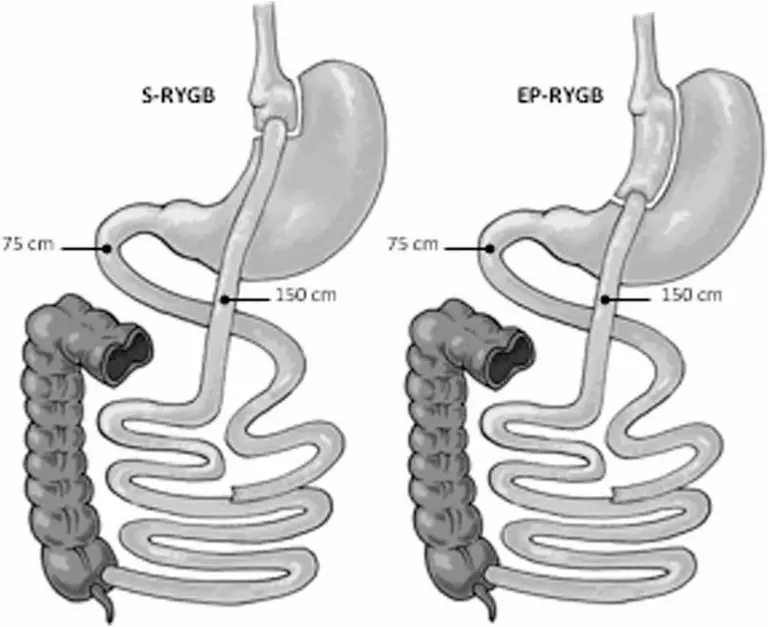
The researchers hypothesised that a narrow longer pouch could lead to better results by preventing pouch dilatation and slowing down gastric emptying rates. They previously conducted a randomised controlled trial (RCT) between September 2014 and October 2015 to evaluate the effect of an extended gastric pouch of 10 cm in a Roux-en-Y gastric bypass (EP-RYGB) compared to a standard 6 cm pouch (S-RYGB).
The underlying hypothesis, supported by LaPlace’s and Poiseuille’s laws, is that a longer, narrower pouch will dilate less, delay gastric emptying, and promote a stronger, sustained feeling of fullness compared to a shorter, wider pouch. These factors may help reduce recurrent weight gain. The three-year results of this trial showed a significant difference of 31% versus 27% in TWL, in favour of the EP-RYGB. This was caused by less recurrent weight gain in the EP-RYGB group.
This latest update is to present the five-to-nine-year outcomes of the previously performed RCT, comparing EP-RYGB versus S-RYGB, in order to determine whether extending the pouch is a gripping point to improve long-term weight loss outcomes and quality of life (QoL) after RYGB.
In the initial trial, 134 patients were randomized into two groups: n = 65 in the S-RYGB group and n = 69 in the EP-RYGB-group. In the S-RYGB group n = 64 received the intervention, and n = 67 in the EP-RYGB group as randomised.
To create the S-RYGB the first blue 60-mm lineal stapler (Echelon, Ethicon, Johnson & Johnson) was placed 5 cm below the angle of His at the right angle to the minor curvature of the stomach. The small proximal pouch was finished using two 60-mm staplers placed against a 40 French stomach tube. The EP-RYGB was created firing the first stapler 10 cm below the angle of His and was finished using three blue 60-mm staplers against a 40 French stomach tube.
For this follow-up study, patients with a known pregnancy in the additional follow-up period (n=1 in the S-RYGB group and n=2 in the EP-RYGB group), patients who were deceased (n=2 in the S-RYGB group and n=2 in the EP-RYGB group), and patients who did not give consent for future research, withdrew from participation, or were lost to follow-up (n=61).
Outcomes
Between November 2023 and October 2024, of the 132 patients in the initial trial, 62 patients were reached and included for long term follow-up. This resulted in a follow-up rate of 47% for both groups (n=30 in the S-RYGB group and n=32 in the EP-RYGB group).
In the analysis of this follow-up study, no significant differences in terms of %TWL were found between the groups in both the crude and the adjusted analyses (p>0.05 for all timepoints).
Maximum TWL at nadir was 34.6 ± 9.2% in the S-RYGB (median 18 [12, 17] months) and 35.5 ± 9.8% in the EP-RYGB group (median18 [12, 17] months] (p=0.71), and 90% in the S-RYGB versus 91% in the EP-RYGB group had reached a TWL of ≥ 20%, postoperatively (p=0.93).
Although not statistically different, more patients in the S-RYGB group tended to experience recurrent weight gain compared to the EP-RYGB group at nine years postoperatively; 70% versus 47%, respectively (p = 0.07).
At baseline, the S-RYGB group tended to have more patients with T2DM than the EP-RYGB group (13 (43.3%) vs. 8 (25.0%), p=0.13. The resolution rates after nine years were similar (46.2% vs. 37.5%, p=0.99). A total of 27 patients (43.5%) were diagnosed with hypertension, of which 15 (50.0%) were in the S-RYGB group and 12 (37.5%) in the EP-RYGB group. The resolution rates after nine years did not differ (66.7% vs. 66.7%, p=0.99). In total, 18 patients (29.0%) were diagnosed with dyslipidaemia.
In the S-RYGB group, 81.9% achieved resolution, compared to 57.1% in the EP-RYGB group (p=0.326). Before surgery, 4 patients (13.3%) in the S-RYGB group suffered from OSAS, compared to 5 (15.6%) in the EP-RYGB group. The resolution rate was significantly different between the groups in favor of the S-RYGB (100% vs. 20%, p=0.048).
HRQoL was comparable between the groups for all domains of the BODY-Q questionnaires (p>0.05 for all). On a scale of 0–100, highest scores regarding HRQoL were found in both S-RYGB and EP-RYGB for the subscales ‘physical activity’ (71 ± 23 vs. 73 ± 20), ‘psychological function’ (62 ± 28 vs. 66 ± 20), and ‘social function’ (67 ± 26 vs. 71 ± 23).
GERD symptoms were low during long term follow-up at 60 (0.5 [0.0, 4.5] vs. 0.0 [0.0, 2.8]) and 109 months (0.0 [0.0, 5.5] vs. 0.0 [0.0, 5.0]). Maximum reported scores were 29 in the S-RYGB group and 35 in the EP-RYGB group, respectively. No significant differences were found at all timepoints mentioned (p>0.05 for all).
The mean score of the Sigstad dumping syndrome questionnaire for both groups was similar (7.0 vs. 7.2, p=0.915). Moreover, the percentage of participants that scored ≥ 7, did not significantly differ between the two groups either (48.3% vs. 40.6%, p=0.61). For the Arts questionnaire, the S-RYGB group had a mean score of 4.3 for early dumping and 2.3 for late dumping, while the EP-RYGB group had a mean of 4.2 for early dumping and 2.3 for late dumping. These differences were not statistically significant (p=0.90 and p=0.99).
“After nine years, EP-RYGB showed a trend towards better weight loss results compared to S-RYGB. Both techniques offer similar outcomes regarding remission of obesity related complications and quality of life improvement. S-RYGB tended to show more recurrent weight gain compared to EP-RYGB,” the researchers concluded. “Due to a high loss of follow-up, these findings should be considered exploratory, and definite conclusions on the long-term advantages of EP-RYGB are subject of future studies with larger sample sizes.”
The findings were reported in the paper, ‘Extended Versus Standard Pouch in Roux-en-Y Gastric Bypass: Five To Nine Year Follow-Up Results of a Randomized Controlled Trial’, published in Obesity Surgery. To access this paper, please click here


Comments