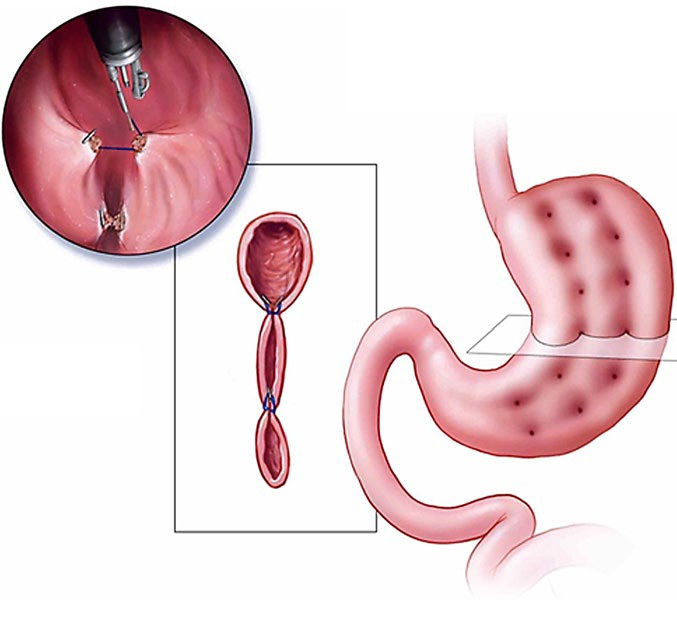
Improving our understanding of endoscopic sleeve gastroplasty
- owenhaskins
- May 5
- 11 min read
The British Obesity & Metabolic Specialist Society (BOMSS) recently revealed that endoscopic sleeve gastroplasty (ESG) procedural data will be incorporated into the Society’s National Bariatric Surgery Registry (NBSR). In this interview, Mr Omar Khan, Chair of the NBSR Committee, and Mr Jamie Kelly, who has performed over 500 ESG procedures, discuss the importance of the registry, why ESG plays a crucial role in the armamentarium of a bariatric specialist and the future possibilities of concurrent bariatric therapies...

“The NBSR was originally set up as an audit tool in 2008 to record bariatric operations and originally it was voluntary. However, to bring the NBSR in line with the regulatory environment, in 2013 it became mandatory for all data from all NHS bariatric cases to be collected and reported to the registry. Since 2013, this data has been used to produce a yearly report on consultant outcomes (Consultant Outcome Publication). The idea is that we produce data which shows the outcomes of individual consultants and individual units,” explained Mr Khan, a Consultant Surgeon at St George's University Hospitals NHS Foundation Trust, London. “That's the audit aspect of the NBSR, but there's an increasing aspect in which we're trying to use the database to potentially answer prospective and retrospective research questions.”
The first iteration of the NBSR recorded data on gastric bands, sleeve, bypass and biliopancreatic diversion with duodenal switch (BPD/DS) operations. Over the years, the registry has evolved to include additional procedures such as gastric balloons and one anastomosis gastric bypass, reflecting the changes in real-world bariatric practice.

“We have always been quite proactive in the NBSR so that it includes newer procedures. Originally, the NBSR was a surgical registry as part of BOMSS, which was then a surgical society. Now that BOMSS is no longer just a surgical society, it's a metabolic specialist society, we are now looking to expand our repertoire of activity and we're also looking to expand our membership, for all practitioners who treat obesity. We are eager that the NBSR captures as much data as possible and one of the barriers for us collecting ESG data was that gastroenterologists who were doing this procedure, were not members of BOMSS. Now that we've made it quite explicit with our name change that we're no longer a surgical society, but a specialist society, we thought this was a good opportunity to try and emphasise that. And one of the ways we're doing that is by trying to emphasise the non-surgical endoscopic aspects of our registry.”
The ESG part of the NBSR, like other procedures on the registry, will record patient demographics, the number of procedures, outcomes (eg weight loss) and complications, as well as which specialists are performing ESG.
“Established procedures such gastric sleeve and bypass have been around for about 20 to 30 years, and so an awful lot of the research questions have been answered. Including ESG into the NBSR, now give us an opportunity to actually get some more detailed information on the quality of life (QoL) post-ESG, so we are adding a significant amount of additional QoL information regarding this procedure. The aim is to try and work with industry, not only to say the procedure is safe, but to do some detailed QoL analysis. Data entry is voluntary and every data field does not have to be filled in, but we're encouraging people to complete as much of the dataset as possible, as part of this prospective audit.”
Mr Khan believes ESG is going to be an important part of the armamentarium of a bariatric specialist, which includes prescribing obesity management medications (eg GLP-1s), ESG and other endoscopic techniques, as well as surgery.
“One of the things that we've realised, particularly in the era of GLP-1s, is we need to get away from this idea that there's one size fits all, and also need to get away from the idea that patients can have either a sleeve or a bypass or an ESG or medication. I would say ESG is part of the spectrum of interventions that we can offer. We still do not really know which obesity treatment/s, is suitable for which patient. What I would say is that ESG fits in the spectrum of interventions, starting with the lower risk interventions such as diet and exercise, then medication, then endoscopic interventions, including ESG, and then bariatric surgery.”
He believes that ESG can be effective treatment in some special cases, such as revisional surgery or for patients presenting with dumping syndrome or weight recurrence after surgery. In addition, there are also a group of patients who want GLP1 therapy, who are not keen on surgery, but are intolerant of GLP1 therapy. For this group of patients, Mr Khan stated it’s really important that he is able to offer patients additional therapies, other than surgery, which they do not want.
“Ultimately, I think it is safe to say that in the longer term the weight loss results from surgery are likely to be better, than ESG, in the same way we can probably say that in the longer term the gastric bypass results are slightly better than the sleeve because it's a bigger and more invasive operation. So, for me, it's a risk-reward scenario. I think the whole notion of individualised care is to offer patients options and discuss with them where they want to go within that spectrum.”
A surgeon’s experience
“I started endobariatic procedures in 2009 in the UK going on to perform ESG using the Overstich device in 2014. It was a strange time because I had a belief and faith in the procedure, but I was the only one doing it in the UK for about six or seven years. Over time, as more and more data was published demonstrating the excellent safety profile and positive outcomes from ESG, more of my surgical and gastroenterological colleagues became interested in the procedure,” explained Mr Kelly, an Upper Gastrointestinal Surgeon at University Hospital Southampton NHS Foundation Trust, Southampton, UK. “For many of us around the world, the notion that this is a very good procedure was ingrained as it offered reproducible weight loss, an excellent safety profile, organ preserving, and patient recovery is faster allowing them to get back to work and other daily activities sooner.”

He noted that there was a particular increase of surgeons interested in ESG after the February 2024 decision by the UK’s National Institute for Health and Care Excellence (NICE) that declared ESG as a safe and effective minimally invasive treatment for obesity1.
“The NICE declaration was important, not only because it considered all the available evidence and found ESG using the Overstich device was safe and effective, but also because the decision meant the UK was the first country in the world endorse ESG as a publicly-funded procedure. Collecting UK data on ESG in the NBSR is so important, so we can understand real world outcomes in the UK patient population, develop prospective trials, but it should also provide a further evidence base enabling the wider global adoption of ESG.”
According to Mr Kelly, the procedure offers several benefits both in terms of the type of surgery and the long-term implications for patients. One of the most important considerations for patients is that ESG is organ preserving and does not involve rerouting the digestive system or bypassing parts of the small intestine. Therefore, patients who undergo an ESG are less likely to experience malabsorption and associated nutrient deficiencies, promoting their overall health and well-being.
“Unlike more invasive procedures such as a gastric bypass or sleeve, ESG does not result in long-term nutritional problems, so patients do not require B12 injections or multivitamins.”
The literature demonstrates that ESG results in a significant reduction in total body weight loss, typically between 13-25% or greater2. In addition, Mr Kelly believes that not only has the literature proven that the procedure is safe and effective, but that we are now seeing papers demonstrating the long-term durability of ESG.
A recent paper by Lahooti et al3, assessed the long-term efficacy, safety and durability of ESG for treatment of obesity ten years post-procedure. The results suggest that ESG is effective and safe for treatment of obesity, with durable long- term results for at least up to ten years after the procedure. The paper concluded, “This procedure should be considered as a dependable option for treatment of obesity particularly among individuals who have not attained their desired results through lifestyle modifications and those who are not eligible for or choose not to undergo bariatric surgery.”
“So, we do have a growing body of evidence to support the long-term effectiveness of the procedure. In many ways, ESG has taken the tried and tested route of previously untested surgical procedures,” he explained. “At first the procedure is doubted for lack of clinical evidence, then there are case studies, randomised controlled trials and meta-analyses. There's lots of data to 3, 4, 5 years out and now there is ten-year data out there as well. If you look in the literature, there's over 17,000 peer review articles on ESG, that's a huge irrefutable body of evidence.”
He added that unlike other more invasive surgeries, ESG has significantly fewer procedure-related complications (eg. leaks, bleeds).
“For serious complications, the return to theatre rate for a sleeve gastrectomy is around 0.5 to 1% in the first two weeks post operatively, compared to less than 0.01% for ESG. Most procedure-related ESG complications are related to the full thickness suturing through the stomach wall. A blood vessel could be damaged causing a bleed, the needle could introduce infection into the abdominal cavity or, in very rare cases, damage the surrounding organs. Reviewing the first 20years of the literature damage to the gallbladder lying anterior to the stomach wall has only occurred in three cases out of more than 70,000. Major adverse events are very rare and can be mitigated further by operative technique.”

The reason such instances are so rare is because surgeons, gastroenterologists and endoscopists, are taught how to correctly perform the procedure. Mr Kelly explained that during the procedure one draws the stomach into the device so that when one sutures, the suture is away from other organs. Furthermore, if a bleed does occur, it is not different from surgery, the operators can keep stitching and ‘snug’ the stitch down tight, to stop the bleeding.
“The other lesson we learned early on was to give those patients prophylactic antibiotics because you are potentially disseminated bacteria into the abdominal cavity, increasing the risk of infection.”
Patients can develop significant debilitating gastro oesophageal reflux following laparoscopic sleeve gastrectomy, however, Mr Kelly stated that ESG actually improves reflux rather than making it worse. He noticed that while performing ESG’s on patients with small haitus hernias they would be reduced at the end of the procedure. Interestingly, researchers have manometrically measured the length of the oesophagus when performing the procedure.
“They found that the procedure increases the oesophageal length by about 3 centimetres. This is due to the ESG shortening the stomach which in turn pulls the oesophagus back into the abdominal cavity. This gives more intra-abdominal oesophageal length, which is part of the mechanism that helps control reflux. And may reconstitute the angle of His further contributing to reflux control. So, I think that's why we see an improvement in reflux in our patients.”
Like Mr Khan, he has also seen patients who are seeking an alternative treatment due to their intolerance to GLP-1s or do not wish to stay on medications for the rest of their lives, and do not want more ‘radical’ surgery. For these patients, ESG is a more appealing option.
“We were delighted with the NICE Guidelines. Because of the safety profile of the procedure, they dropped the minimum BMI down to 27.5 for certain at-risk groups. It’s useful in patients with a hostile abdomen that might otherwise be excluded from surgery. And due to its organ preserving nature and safety profile ESG can be considered for adolescents. But it’s range does not have to be confined to lower BMI patients. Studies that show super obese patients who were given an ESG initially as a bridge-to-surgery, did so well they did not require additional surgery.”
Looking to the future, Mr Kelly stated that obesity will be treated like cancer with combination therapies, such as GLP-1 plus ESG or surgery with treatment tailored to the patients’ needs and genetics.
“Ultimately, this is a good thing, because it really encourages more discussions and the sharing of ideas between the different specialties involved in obesity and that’s better for our patients in the short- and long-term. However, GLP-1s are not for everyone and if you look at the data from the GLP1 trials, the serious adverse event ratio is between 4 to 9%, compared to ESG with a serious adverse event ratio of about 1 to 2%. There is also a significant discontinuation rate because of the side effects of the drugs.”
Tips and tricks
Mr Kelly then offered some words of wisdom on how best to carry out ESG procedures, how best to avoid complications and optimise patient outcomes from his years of experience.
“Patients need to be set up to succeed, MDT input and counselling a patient as to how the procedure works is essential. From an operative side of things, Boston Scientific deliver online training, hands-on training and then the first ten cases in the UK are proctored so that the patients are very safe. This also optimises outcome for the patients, as they do not get trapped in an operator’s learning curve with a suboptimal outcome.”
He added that it is important for the operator to appreciate their learning curve and minimise their cases initially to two-a-day. It is crucial that trainees give themselves the time to learn.
Contraindications
Like all surgical procedures, there are several contraindications to ESG, however, whilst initially working with the Overstitch Advisory Board, Mr Kelly said there was a long contraindications list, overtime this was reduced as knowledge on the safety profile of the procedure increased.
“It is important to note that our knowledge on contraindications is changing, for example, we would of initially excluded liver transplant patients due to their immunosuppression. But in some transplant patients weight gain is leading to graft rejection. In this setting the benefit of an ESG potentially exceeds risk and the weight loss will preserve the transplanted liver”
Cost-effectiveness
As intimated earlier, one crucial element of incorporating the ESG procedure into the NBSR is to examine the cost-effectiveness of the procedure. There have been several papers, both in the US and UK, that have reported it is cost-effective for healthcare providers and this could have significant implications for the adoption of ESG by healthcare systems across the world. One such paper by Kelly et al4, was the first cost-effectiveness analysis of ESG versus lifestyle modification (LM) alone in adults with class II obesity (BMI 35.0–39.9 kg/m2) from a national healthcare system perspective in England. The outcomes indicated that ESG was highly cost effective versus LM alone and that, “In the context of rationed access to NHS-funded bariatric services for obesity, availability of an effective and safe intervention that can be routinely delivered as a day case procedure would represent a valuable addition to complement current routine practice.”
“Overall, we need to be guided by the science and I believe ESG has been proven to be safe and effective, delivering durable long-term outcomes,” Mr Kelly concluded. “I look forward to contributing our ESG data to the NBSR so we can learn more about the effectiveness of the procedure and how we can use the data to treat more patients with obesity.”
Further information
For more information on the Bariatric Endoscopic Weight-Loss Treatments, offered by Boston Scientific, please visit here
References
Endoscopic Sleeve Gastroplasty for Obesity, National Institute for Care and Excellence, February 2024
Abu Dayyeh BK, Bazerbachi F, Vargas EJ, Sharaiha RZ, Thompson CC, Thaemert BC, Teixeira AF, Chapman CG, Kumbhari V, Ujiki MB, Ahrens J, Day C; MERIT Study Group; Galvao Neto M, Zundel N, Wilson EB. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity (MERIT): a prospective, multicentre, randomised trial. Lancet. 2022 Aug 6;400(10350):441-451. doi: 10.1016/S0140-6736(22)01280-6. Epub 2022 Jul 28. PMID: 35908555.
Lahooti, Ali BS1,*; Rizvi, Anam MD1; Baig, Muhammad Usman. MBBS1; Akagbosu, Cynthia MD, MA1; Mahadev, SriHari MD2; Sampath, Kartik MD1; Carr-Locke, David L. MA, MD, FACG1; Aronne, Louis MD1; Shukla, Alpana MD1; Johnson, Kate E. BS1; Herr, Andrea NP1; Newberry, Carolyn MD2; Kumar, Sonal MD, MPH1; Sharaiha, Reem MD1. S2063 Ten-Year Outcomes of Endoscopic Sleeve Gastroplasty for the Treatment of Obesity. The American Journal of Gastroenterology 119(10S):p S1473-S1474, October 2024. | DOI: 10.14309/01.ajg.0001037620.30740.d4
Kelly, J., Menon, V., O’Neill, F. et al. UK cost-effectiveness analysis of endoscopic sleeve gastroplasty versus lifestyle modification alone for adults with class II obesity. Int J Obes 47, 1161–1170 (2023). https://doi.org/10.1038/s41366-023-01374-6

Comments